Person, Place, and Time
Who gets it?
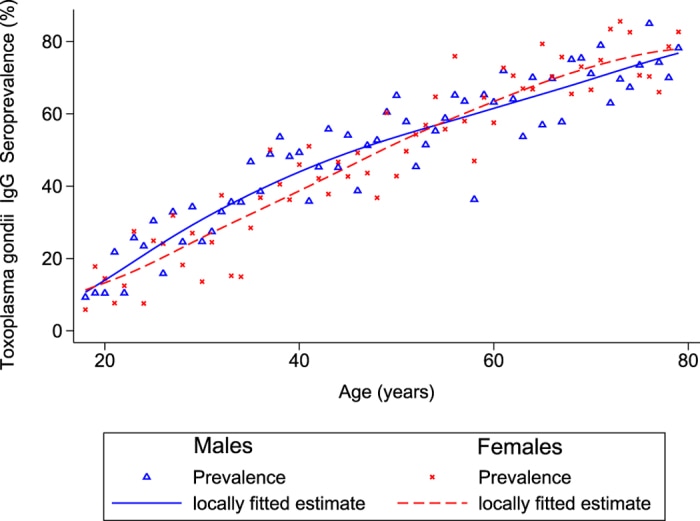
Anyone can get toxoplasmosis but risk is higher for people who have regular contact with cats, have a BMI≳30, or live in rural areas. Additionally, increased risk of contracting the parasite has also been shown to increase with age [12]. The CDC estimates that ~11% of the U.S. (over 6 years of age) is infected with the parasite; exposure in other countries however can reach up to an estimated 95% of the population [1]. A study of Toxoplasmosis prevalence in Germany found that prevalence is also slightly higher among young men and older women [12].
Anyone can get toxoplasmosis but risk is higher for people who have regular contact with cats, have a BMI≳30, or live in rural areas. Additionally, increased risk of contracting the parasite has also been shown to increase with age [12]. The CDC estimates that ~11% of the U.S. (over 6 years of age) is infected with the parasite; exposure in other countries however can reach up to an estimated 95% of the population [1]. A study of Toxoplasmosis prevalence in Germany found that prevalence is also slightly higher among young men and older women [12].
|
Figure 9 Comparison of IgG seroprevalence levels within German citizens shows a slightly increased likelihood of infection in men. The study, conducted from 2008-2011 in Germany also shows an increased prevalence of IgG antibodies against the parasite in older populations. |
One study, conducted in France (2007) using laboratory analysis and recording of possible congenital toxoplasmosis cases within its population, calculated the occurrence of the disease via gestational age and age of the mother [17]. In these representations congenital toxoplasmosis was recorded more frequently in fetuses ranging from 29-32 weeks (Figure 10), and overall occurrence of the disease per 1,000 live births ranged from 0.18-.57 within the population (Figure 11) [17]. While these numbers seem small in comparison to the population of a country such as France, the overall prevalence/occurrence of this parasitic disease is still much more common than one would like to observe in both developed and third world countries.
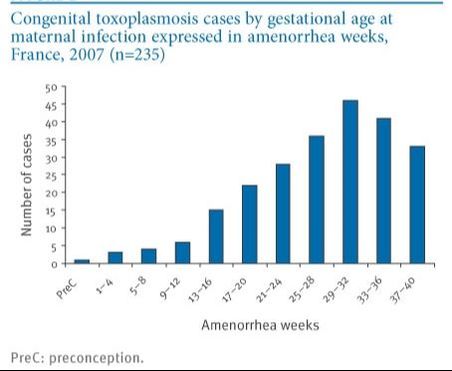
Figure 10 Graphical depiction of reported congenital toxoplasmosis cases during yearly period in France shows a correlation between gestational weeks and number of clinical cases. In this study, the highest number of reported cases occurred during the 29-32 week period of pregnancy [17].
|
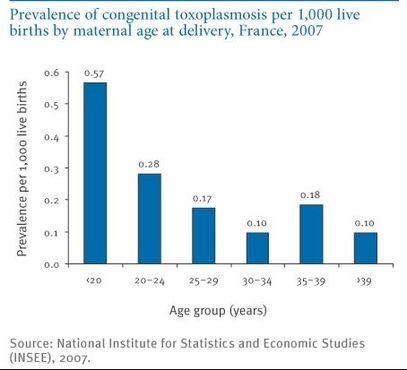
Figure 11 congenital toxoplasmosis cases per 1,00 live births in France. increased rates of the disease were seen in pregnant women below the age of 20 (0.57), increased maternal age appeared to significantly affect the likelihood of congenital transmission of the parasite [17] .
|
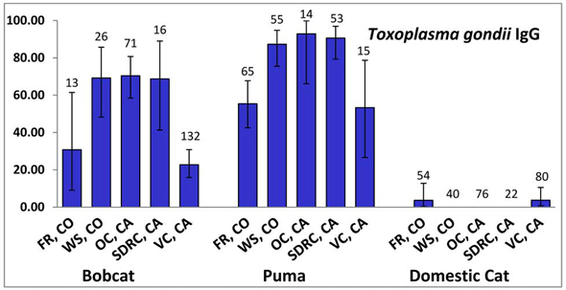
Figure 12 A study which testes wild bocat, puma, and domesticated cat populations (in CA, CO) shows a varying range of IgG (antibody) prevalence across populations. Overall domesticated cats were shown to have relatively low prevalence of infection, while wild cat samples had distinctly higher IgG levels [18].
|
Parasite prevalence in cats ranges depending on geographical location; in one study conducted on wild/domestic cats throughout California and Colorado, domesticated cats had a relatively low prevalence (~5-10%) [18]. However, various other studies have previously reported prevalence of toxoplasmosis as high as 35% within cat populations across the country [18] . Overall, estimates of the total umber of cats infected with the parasite vary widely not only between studies, but also region.
|
Ethnicity and Other Factors
In general, contact with cats is the main distinction between increased and lower risk of contracting toxoplasmosis. There seems to be no definable trend between ethnicity differences other than those who live/have lived in regions with higher population of domestic/wild cats.
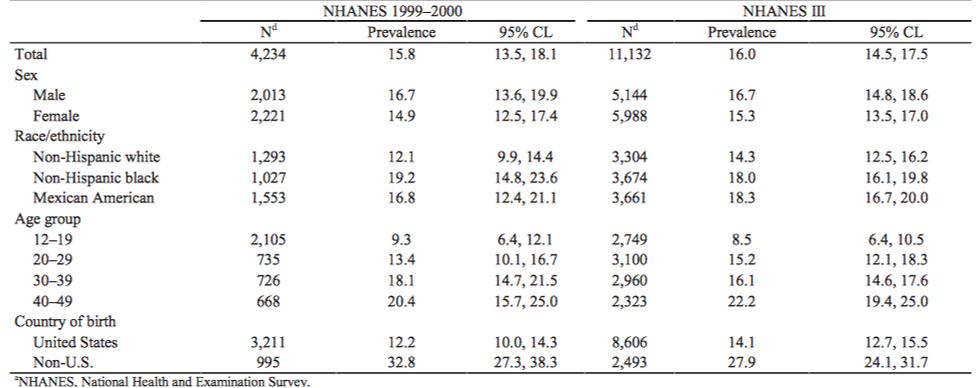
Figure 13 Overall, higher prevalence of toxoplasmosis / Toxoplasma gondii infection is seen in increasing age groups. Ethnicity differences (in the U.S.) do not appear to be a significant factor affecting risk of infection; however, there is a significant increase in prevalence (32.8%) in those who were not born within the U.S. (almost a two-fold increase is seen) [1] .
Environmental Factors
Where does it occur?
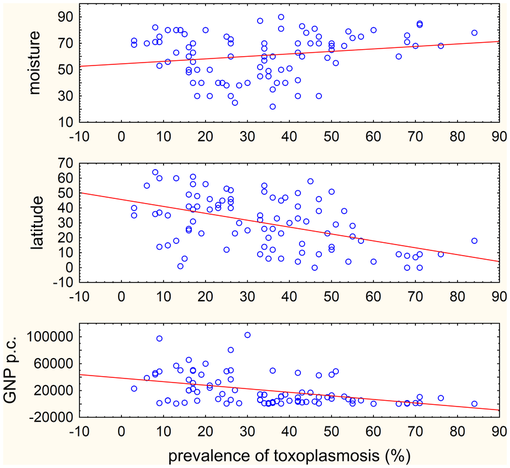
Although 25-30% of the world population has been infected, distribution varies widely. Low prevalence is observed in North America, Northern Europe, Southeast Asia and the Sahelian countries of Africa. While moderate prevalence is seen in Central and Southern Europe and High prevalence is seen in South America and tropical African countries [14] . Highest prevalence is seen in moist, warm climates. There is also a correlation between prevalence and low GNP [15] .
Although 25-30% of the world population has been infected, distribution varies widely. Low prevalence is observed in North America, Northern Europe, Southeast Asia and the Sahelian countries of Africa. While moderate prevalence is seen in Central and Southern Europe and High prevalence is seen in South America and tropical African countries [14] . Highest prevalence is seen in moist, warm climates. There is also a correlation between prevalence and low GNP [15] .
|
Figure 14 prevalence of toxoplasmosis infection varies with geographical location, specifically dealing with warmer, more humid environments. Overall as latitude decreases, prevalence of infection tends to increase, while the increase in moisture levels point towards higher levels of infection [15] .
|
When does is occur?
While no significant trend is observable in the prevalence of T. gondii infection throughout the year (no definable pattern such as the flu), slightly higher rates of occurrence can be observed during warmer months. One study conducted on pregnant women seeking medical treatment at Brazilian clinics in the city of Divinopolis (2007-2008) pointed towards an increased seropositive test (Ig and IgM) in individuals in the months of May, June, and July; overall differences throughout the entire population however appear to be minimal [16] .
While no significant trend is observable in the prevalence of T. gondii infection throughout the year (no definable pattern such as the flu), slightly higher rates of occurrence can be observed during warmer months. One study conducted on pregnant women seeking medical treatment at Brazilian clinics in the city of Divinopolis (2007-2008) pointed towards an increased seropositive test (Ig and IgM) in individuals in the months of May, June, and July; overall differences throughout the entire population however appear to be minimal [16] .
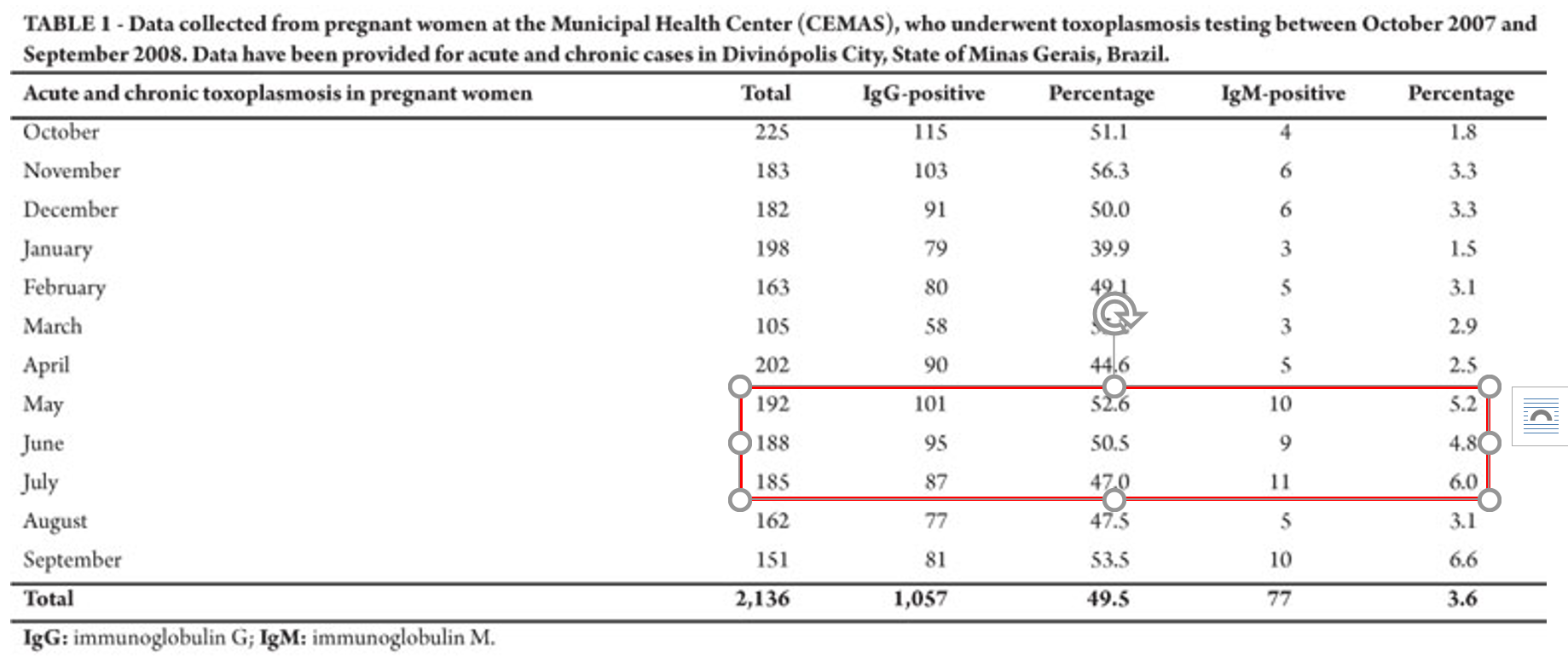
Figure 15 In a study conducted in Brazil, slightly increased rates of toxoplasmosis prevalence (in women attending clinical check-ups) was seen in hotter months. The months of May, June, and July showed increased occurrence of T. gondii infections within the study population, with the most notable increase seen in July. IgG (antibody) positive tests were recorded in ~40-50 of the women, while IgM positive results were seen in only ~5-6% of women [16] .
